Polycystic Ovarian Syndrome (PCOS)
What is PCOS?
PCOS is a hormone imbalance in women that impacts 1 out of 10 to 15 women. PCOS probably has several etiologies (ovary, adrenal, pituitary and hypothalamus) and has gradients from mild to severe. PCOS is part of the metabolic syndrome which includes insulin resistance, abnormal lipid measurements, obesity, high blood pressure, acne, facial hair growth, infertility, male pattern balding and weight loss difficulty.
What are the signs of PCOS?
Common signs include no periods, irregular periods, or heavy periods. Other symptoms include pelvic pain, weight gain or trouble losing weight, acne, and thick skin with dark patches. Half of women with PCOS will experience weight gain and many experience issues with fatigue and difficulty sleeping. Middle age women experience hair loss. Additionally, many women experience mood changes because of PCOS.
Diagnosis of PCOS
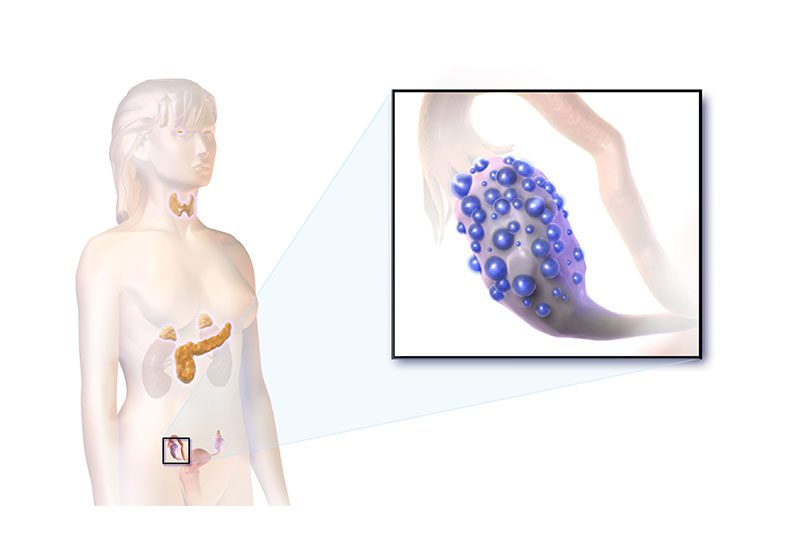
For the diagnosis of PCOS, Endocrinologists such as Dr. Friedman will test for high serum androgen levels, especially bioavailable testosterone, and insulin-resistance based on SHGB (Sex hormone binding globulin) and to a lesser extent, HbA1c or insulin levels. Gynecologists rely more on seeing ovarian cysts (often in a string of pearls pattern) on ovarian ultrasound. Since other endocrine conditions can present similar symptoms like PCOS, laboratory testing is crucial for diagnosis. Testosterone is usually high in polycystic ovarian syndrome, especially the bioavailable testosterone, while it is usually low in other endocrine diseases like Cushing’s syndrome or hypopituitarism.
SHGB (Sex-hormone binding globulin) is a protein that is made in the liver that binds to both testosterone and estradiol. SHBG varies widely among women
Total testosterone includes SHBG-bound testosterone (which is inactive) and free testosterone and albumin-bound testosterone. Bioavailable testosterone which is an active form of testosterone includes free testosterone and albumin bound testosterone. When SHGB is low, the level of bioavailable testosterone increases and when SHGB is high, the level of bioavailable testosterone decreases. SHGB is reduced with insulin resistance and obesity which are the common findings among women with PCOS. Birth control pills and other forms of oral estrogen raise SHGB, therefore raising total testosterone. The effects last over a year even after stopping birth control pills. However, SHBG is not affected by transdermal estrogen such as Estrogel or an Estradiol patch. If a woman is not on birth control pills or oral estrogen, a high SHBG is good and indicates less insulin resistance.
Other hormones use to diagnosis PCOS are LH/FSH (a ratio > 3:1 is consistent with PCOS) and DHEAS which is also often high in PCOS. Measuring an estradiol and FSH/LH are helpful to determine menopausal status, prolactin (to look for a prolactinoma and 17-OH progesterone (to
look for congenital adrenal hyperplasia (CAH) are helpful to exclude other diseases that give menstrual abnormalities.
Other hormones use to diagnosis PCOS are LH/FSH (a ratio > 3:1 is consistent with PCOS) and DHEAS which is also often high in PCOS (especially an adrenal variant of PCOS). Measuring an estradiol and FSH/LH are helpful to determine menopausal status, prolactin (to look for a
prolactinoma and 17-OH progesterone (to look for congenital adrenal hyperplasia (CAH) are helpful to exclude other diseases that give menstrual abnormalities.
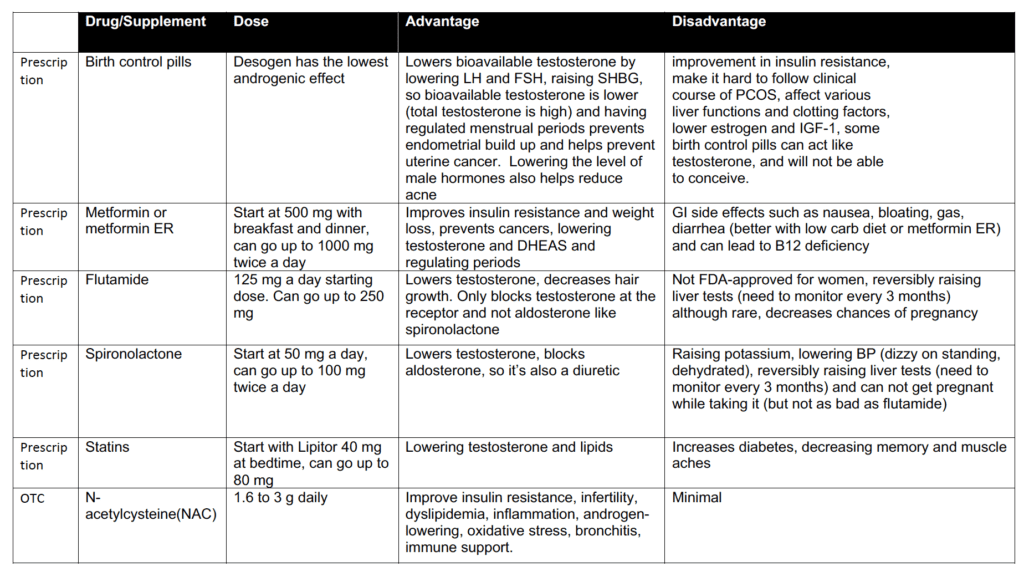
Treatment for PCOS (see Table)
There are many treatment options for PCOS. Birth control pills are commonly used for PCOS treatment and is recommended by the Endocrine Society. Advantages of birth control pills are helping lower bioavailable testosterone by lowering LH and FSH, and raising SHBG, so bioavailable testosterone is lower (total testosterone is high) and having regular menstrual periods that prevents endometrial build up and helps prevent uterine cancer. Lowering the level of male hormones also helps reduce acne. Disadvantages there are no improvement in insulin resistance and since periods are induced artificially, it is hard to follow the clinical course of PCOS. Birth control pills can also affect various liver functions and clotting factors, and lowers estrogen and IGF-1. Some birth control pills can act like testosterone, and women will not be able to conceive.
Dr. Friedman recommends using metformin. Start with 500 mg once daily at dinner or bedtime, increase to twice a day after two weeks, and can go up to a maximal dose of 2000 mg/day. Metformin ER can be used if side effects to metformin occur. Advantages of metformin include improvements in insulin resistance and weight loss, preventing cancers, lowering testosterone and DHEAS, and regulating periods. Disadvantages are GI side effects such as nausea, bloating, gas, diarrhea (better with low carb diet or metformin ER) and can lead to B12 deficiency.
Another medication frequently used in combination with or without metformin is flutamide. It is FDA-approved for prostate cancer and not for PCOS, however it both lowers and blocks the action of testosterone and helps with symptoms of PCOS related to high testosterone. Advantages are: lowering testosterone, decreasing hair growth, and only blocking testosterone at the receptor and not aldosterone, like spironolactone. Disadvantages are: not FDA-approved for women, reversibly raising liver tests (need to monitor every 3 months). Women should not get pregnant while taking the drug.
Spironolactone is another drug of choice that blocks and lowers testosterone. Advantages are: lowering testosterone and is also a diuretic (water pill) which can decrease swelling and water weight), it also blocks aldosterone at the aldosterone receptor unlike flutamide. Disadvantages are: raising potassium, lowering BP (dizzy on standing, dehydrated), reversibly raising liver tests (need to monitor every 3 months). Women should also not get pregnant while taking the drug, although it is probably safer in pregnancy than flutamide.
Statins are also a useful drug to lower testosterone in PCOS. All statins (Lipitor, Crestor, Simvastatin) can be used, although Lipitor (atorvastatin) is what Dr. Friedman typically uses. Advantages are: Lowering testosterone and lipids. Disadvantages are increasing blood sugar levels and muscle aches, and rarely decreased memory.
GLP-1 receptor agonists are diabetes medicines that lower testosterone in PCOS. These are often expensive and may not be covered if the patient doesn’t have diabetes. With the exception of Rybelsus, these are all subcutaneous shots (in your stomach with a small needle). Dr. Friedman usually prescribes Semaglutide (Ozempic) with Liraglutide (Victoza) and dulaglutide (Trulicity) also options depending on insurance coverage. Advantages are: Lowering testosterone weight loss, improved diabetes parameters. Disadvantages high cost if not covered by insurance. Side effects include nausea, vomiting, abdominal pain, loss of appetite, diarrhea, constipation.
All these treatments help regular menstrual cycles and reduce male hormones (testosterone and DHEAS). Often PCOS patients need to use more than one drug due to drug side effects and need dietary supplement intervention.
PCOS Complications
It is important to monitor for weight gain, pre-diabetes, diabetes, endometrial cancer, and metabolic syndrome. Metabolic syndrome is a collection of symptoms; impaired glucose, high blood cholesterol, abdominal obesity, and high blood pressure. Women with PCOS have a 4 to 7 times higher risk of developing prediabetes and type 2 diabetes. PCOS does not cause endometrial cancer, but having infrequent or no periods increases the risk.
Healthy PCOS diet and Supplements
Weight loss and healthy diet is crucial for PCOS treatment. Start the day with a high protein breakfast. Eat regular meals and snacks throughout the day. Include protein, fat, and a small amount of complex carbohydrates at meals and snacks. Focus on unprocessed whole foods and include an assortment of vegetables. Divide carbs and protein to one-quarter of your plate and half of the plate with fruits and vegetables. Avoid starchy processed carbohydrates such as cereals, white bread, white rice, baked goods, crackers, candy, and sugary drinks. These will increase insulin release and trigger inflammation.
Treatment may include supplements as well. Certain supplements help improve insulin, cholesterol, and triglycerides levels. Others lower testosterone and DHEAS. Furthermore, they promote ovulation and increase egg quality. It is important to replace nutrients that are missing from your diet due to malabsorption or diet avoidance. Optimizing nutrient levels is also critical. Commonly used supplements are Vitamin B12, which is often deficient in metformin users over the time, PCOS patients who take metformin should have their vitamin B12 levels checked annually and supplement their diets with vitamin B12. Recommended levels > 400 pg/mL of vitamin B12, and replacement of 1000 mcg a day is recommended if low
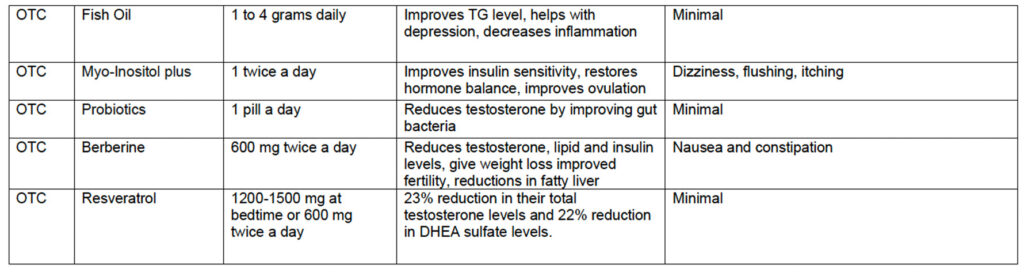
N-acetylcysteine (NAC), which is Antioxidant and amino acid derivative from L-cysteine, a precursor to glutathione. Advantages are: improves insulin resistance, infertility, dyslipidemia, inflammation, androgen-lowering, oxidative stress, bronchitis, immune support. Recommended dosage: 1.6 to 3 g/day although obese women need more than 3g/day to be effective. Disadvantages are: fairly expensive. Make sure you order NAC and not another supplement with a similar name. Recommended brand on Amazon: NAC from NOW, 1000 mg 3X/day.
Fish oil (1000 mg twice a day) Advantages are: reducing inflammation, helping with depression, and supporting healthy pregnancy. Disadvantages are minimal to using fish oil, although some patients do not like the taste. Recommended brand on Amazon: Nature’s Bounty Fish Oil, 1000 mg twice a day.
Myo-Inositol(MYO) (2000 mg) and D-chiro-Inositol (DCI) (50 mg) (available on Amazon as Myo-Inositol plus) are relatives of the B-complex vitamins and mostly found in foods (fruits, beans, cereals, buckwheat, etc.). Advantages are: improves insulin resistance, dyslipidemia, androgen-lowering, infertility, hypertension, weight loss, increase good cholesterol, reducing gestational diabetes risk, and improving egg quality in PCOS. Disadvantages are: hypoglycemia. Recommended brand on Amazon: Myo-Inositol plus from Omnibiotics, 2000 mg/50 mg once a day.
Resveratrol (600 mg twice a day) is an antioxidant with anti-aging, anticancer, and cardioprotective properties. Found in the skin of grapes, berries, red wine, and peanuts. Advantages are: reduction in total testosterone levels and DHEA sulfate levels. Disadvantages are Gastrointestinal distress. Recommended brand on Amazon: Drs. Best Trans-Resveratrol, 600 mg twice a day. Or Nutrivein Premium Resveratrol, 725 mg twice a day.
Probiotics (1 pill a day) have recently been found to lower testosterone and improve PCOS symptoms. Dr. Friedman does not recommend any particular brand.
Summary
In PCOS, diet and nutrition modifications complement medical therapy. Anti-inflammatory foods, sensible portions, and low carb intake is essential. Nutrition supplements when added to a healthy diet and lifestyle can offer health benefits and aid in improving ovulation. More randomized clinical trials are needed to determine benefits of supplement use in women with PCOS. Women with PCOS should discuss the health benefits/risks of supplement use, appropriate dosage, and be monitored by a healthcare professional.